Introduction:
Oral cancer in an ideal cancer to identify early by screening[1]. Studies have shown that oral cancer can be silent in symptomology with awareness of early signs being more beneficial in diagnosis[2]. The incidence of oral cancer is increasing[3] with 4,19,000 new cases diagnosed annually world wide[4]. Despite the advances in therapeutic management and increased understanding of the molecular basis of disease, survival rates have not improved in the last few decades, the 5 year survival rate is 50%[5] mostly because of the advanced stage at diagnosis[6]. However, early diagnosis of oral cancer greatly increases the probability of cure with minimum impairment and deformity[7]. Epidemiologic studies suggest that early detected disease has a relative survival rate of 82% but this reduces to 32% due to dental practitioners negative attitude and low level of knowledge that contributes to delayed or inadequate detection of early stages of oral cancer (Sadowsky et al, 1998; Schnetler, 1992; Shafer, 1975).
Early, curable stages of oral cancer are small, asymptomatic lesions8 that may be easily missed by the patients, highlighting the important role of dentists in reducing the burden of oral cancer.
Dentists are qualified to opportunistically screen for oral cancer and to provide preventive advice and counseling during routine examinations. It is vital that dentists have accurate knowledge about oral cancer to identify individuals at risk, examine the mouth to document tissue changes and provide appropriate interventions. Thus dentists can play a crucial role in the reduction of oral cancer incidence, morbidity and mortality. With this background; the purpose of this study was to assess the GDPs’ awareness of prevention and early detection of oral cancer.
Materials And Methods
The cross - sectional survey was conducted between February 2013 to May 2013, among a random sample of 100 general dental practitioners (GDPs’) in Amritsar district. The self-administered anonymous questionnaires used for this study were handed out, to the general dental practitioners with an information sheet which explained the purpose of this project. Participation was on voluntary basis and all respondents were clearly advised that participation was anonymous and they had the right to comply with or refuse participation. Response to the questionnaire constituted the participants informed consent. The questionnaire was designed to test the GDPs’ knowledge of oral cancer under 3 main categories:- 1) knowledge of risk factors, 2) knowledge of clinical diagnostic concepts and 3) current diagnostic practices of oral cancer followed by them. The responses were elicited in either categorical ‘yes’, ‘no’ options or in MCQ (multiple choice questions) format with one correct answer. The completed questionnaires were then entered in SPSS version 17 for statistical analysis. The responses were coded as numeric in order to facilitate the data entry. The results were analyzed using Pearson chi-square (χ2) test.
Results:
From a total of 100 questionnaires distributed, 84 general dental practitioners returned completed questionnaires giving a response rate of 84%. Vast majority of respondents were males (85.7%). Mean age of the respondents being 35 years and the mean number of years since graduation was 18. Demographic characteristics of the respondents shown in (Table 1).
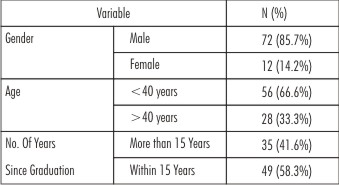 | Table 1 : Demographic Characteristics Of Respondents (N=84)
 |
Knowledge of Risk Factors:
The results of our study showed that tobacco smoking and smokeless tobacco use (100%) were considered as the most potential risk factors for oral cancer by the general dental practitioners, followed by betel quid chewing (96.4%; n=81) as the second most important risk factor. Prior oral cancer lesions (94%; n=79) and alcohol use (86.9%; n=73) were identified as third and fourth key risk factors respectively. However, lower numbers reported U.V. exposure (69%), older age (64%), viral infection (57.1%) and low consumption of fruits and vegetables (26.1%) as risk factors of oral cancer. Knowledge of risk factors shown in (Figure 1).
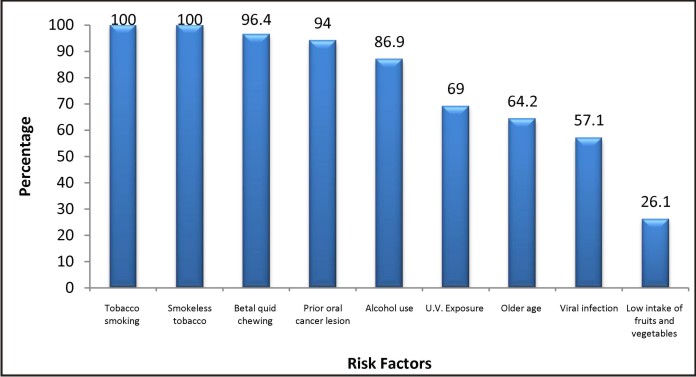 | Figure 1 : Knowledge Of Risk Factors
|
Knowledge of Diagnostic Concepts:
The majority of general dental practitioners (98.8%; n=83) surveyed, agreed that early detection of oral cancer improves its five year survival rate. Patient in usually asymptomatic during the initial stages of the disease was identified by 92.8% (n=78) GDPs’ and 75% (n=63) GDPs’ believed that oral cancer lesions are mostly diagnosed in the advanced stage.
Erythroplakia and leukoplakia were identified as the most common type of lesions associated with oral cancer by 85.6% GDPs’. However, a higher proportion of dentists identified leukoplakia (92.8%; n=78) than erythroplakia (78.5%; n=66) as the most common premalignant lesion .Only 72% of the respondents identified both lesions.
A total of 73.8% (n=62) GDPs’ identified tongue and 88% (n=74) identified floor of mouth as the two most common sites for intra-oral lesions . However, only 64% GDPs’ identified both the sites.
Visual inspection was considered as the most effective screening method by 64.2% (n=54) of the general dental practitioners. Knowledge of diagnostic concepts shown in (Figure 2).
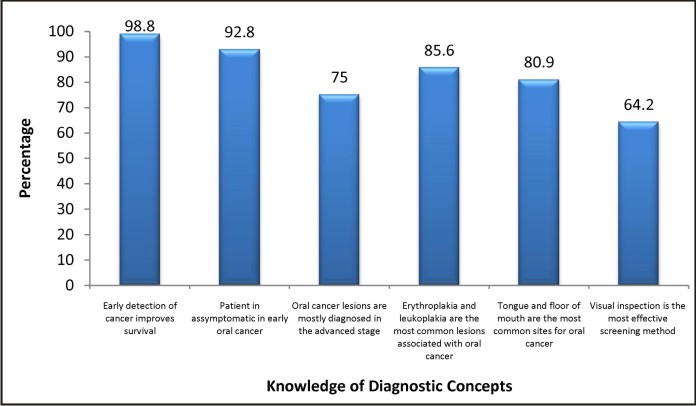 | Figure 2 : Knowledge Of Diagnostic Concepts
|
Current Diagnostic Practices of Oral Cancer:
Of the general dental practitioners 88.0% (n=74) affirmed that they routinely performed systematic examination of the oral mucosa on every patient .It was found that 67.8% (n=57) of GDPs’ routinely asked the patients if they were using tobacco in any form while only 22.6% (n=19) asked the patients about their alcohol intake. Regular advise to the patients about risk factors of oral cancer was delivered by 44.0% (n=37) GDPs’. Regarding the referral of the suspected patients, 94.0% (n=78) GDPs’ suggested an oral and maxillofacial surgeon to be the appropriate person for management of such patient. Percent distribution of GDPs’ according to current diagnostic practice of oral cancer shown in (Figure 3).
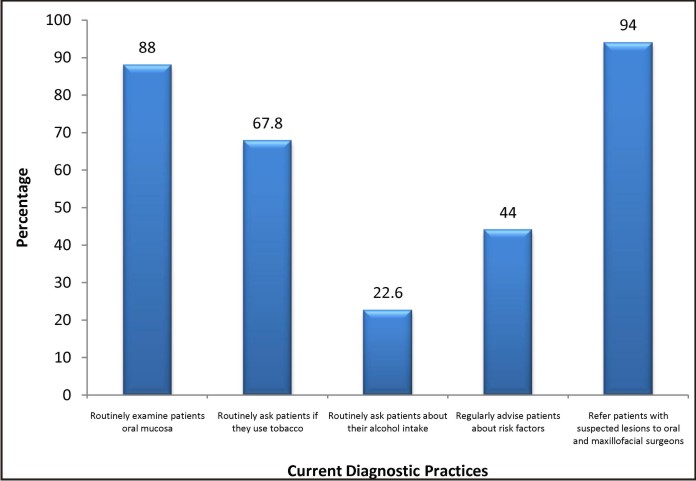 | Figure 3 : Percent Distribution Of Gdps’ According To Current Diagnostic Practices
|
Discussion
A comprehensive oral cancer examination and risk assessment are measures that may lead to early detection and prevention of oral cancer. Many experts agree that the key is not necessarily identifying oral cancer but identifying tissue that is not normal and taking appropriate action[9].
The results of the present study show that general dental practitioners of Amritsar district are generally knowledgeable regarding oral cancer risk factors and diagnostic concepts, however, similar to other studies[10],[11],[12],[13] there is variability in their knowledge. Although the vast majority of dentists identified tobacco, alcohol, betel quid chewing and prior oral cancer lesion as the main risk factors, similar to other studies conducted in the US[10],[11],[14],[15],[16], Canada[12] and Europe[13] a smaller proportion of GDPs’ were aware that viral infection, U-V exposure and low consumption of fruits and vegetables are also potential risk factors of oral cancer. Only 57.1%. of dentists identified older age as a risk factor for development of oral neoplasia. This figure is low in comparison to similar studies carried out in US[10],[14], Canada[12] and Spain[13].
Dentists knowledge of oral cancer diagnostic concepts was found to be better compared to the knowledge of risk factors. The majority of dentists (98.8%) knew that early detection improves survival which is similar to results seen among dentists surveyed in USA[14], Canada[12] and Germany[17]. Three fourths of the dentists knew that oral cancers are most often diagnosed in the advanced stage in contrast to only 50% in most of the other surveys[10],[12],[14],[18]. Oral visual screening can reduce mortality in high risk individual and has the potential to prevent at least 37000 oral cancer deaths per year world wide[19]. In the present study 64.2% of GDPs’ recognized visual inspection as the most effective screening method.
Over 80% of GDPs’ knew that erythroplakia and leukoplakia are the main pre-cancerous lesions associated with oral neoplasia. However, a higher proportion (92.8%) identified leukoplakia is comparison to erythroplakia (78.5%). Although both lesions have malignant potential, erythroplakia, and the red component of erythroleukoplakia, known as speckled erythroplakia, have a greater chance to progress to oral cancer[8],[20]. In addition, it has been reported that on histopathological assessment over half of erythroplakias were invasive carcinoma, and 40% showed carcinoma in situ[21].
Although 88%, GDPs’ considered floor of mouth and 73.8% identified tongue as the most common sites of oral cancer, only 64% recognised both sites as high risk. Similarly some dentists were not aware that the ventral and lateral border of the tongue is a high risk area for suspicious lesions is the case of tongue carcinoma[8],[20].
It has been reported in previous studies that increased referral is significantly associated with greater knowledge of oral cancer[14]. In our study similar finding were obtained, with 94% GDPs’ referring patients with suspected lesions to oral and maxillofacial surgeons.
Inspite of their knowledge of risk factors, in the present study only 67.8%. GDPs’ routinely asked patients about their tobaccos habit. However, dentists should ask the patients about tobacco use and advise in order to ensure early prevention.
In this study only one fifth of the dentists reported that they routinely ask patients about their alcohol intake however, dentists have been encouraged to screen and counsel patients about alcohol use[22].
Although the general dental practitioners present with a good knowledge of risk factors of oral cancer, a relatively small proportion of dentists were found regularly advising the patients about risk factors (only 44% of GDPs’). This finding is similar to the other surveys[15],[16] and suggest that dental practitioners find counseling their patients regarding risk factors as challenging. On the contrary, patients have been found to be receptive of dentists advice on such matters[23]. Therefore, dentists should advocate healthy life style behaviour and actively participate in oral cancer prevention emphasizing the importance of risk factors.
The present study also showed that number of years since graduation and age of dentists are factors which have quite an impact on their knowledge. Although there was no significant difference, the dentists of younger age group and recent graduates demonstrated better knowledge. This emphasizes the need for continuing education (CE) on the topic.
Conclusion
This study highlighted the importance of improving educational methods for general dental practitioners, on oral cancer detection and premalignant lesions of the oral cavity because the dental practitioners are capable of and have an excellent opportunity to bring about positive change in reducing the rising incidence of oral cancer and ultimately saving lives.
References:
1. McGurk M, Chan C, Jones J, O Regan E, Sheriff M. Delay in diagnosis and its effect on outcome in head and neck region. B J OMFS 2005; 43(4): 281-84.
2. Scrully C, Malamos D, Levers BG, Porter SR, Prime SS. Sources and patterns of referrals of oral cancer: Role of general practitioners. BMJ (Clinical research ed) 1986; 293: 65470, 599-601.
3. Gillison ML. Current topics in epidemiology of oral cavity and oropharyngeal cancers. Head Neck 2007; 29(8): 779-792.
4. Ferlay J, Shin H, Forman D, Mathers C, Parkin D. GLOBOCAN 2008. Cancer incidence and mortality worldwide: IARC Cancer Base No. 10, 2010 – http;//globcar.iarc.fr
5. Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Cancer 2009; 45(45): 309-316.
6. Wade J, Smith H, Hankins M, Llewellyn C. Conducting oral examinations for cancer in general practice: what are the barries? Fam Pract 2010; 27(1): 77-84.
7. Joseph BK. Oral cancer: prevention and detection. Med Princ Pract 2002; 11: 32-35.
8. Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin 2002; 52(4): 195-215.
9. Sciubba JJ. Oral cancer and its detection: history taking and the diagnostic phase of management. J Am Dent Assoc 2001; 132: 125-85.
10. Yellowitz JA, Horowitz AM, Drury TF, Goodman HS. Survey of US dentists knowledge and opinions about oral pharyngeal cancer. J Am Dent Assoc 2000; 131(5): 653-61.
11. Applebaum E, Ruhlen TN, Kronenberg FR, Hayes C, Peters ES. Oral cancer knowledge, attitudes and practices: a survey of dentists and primary care physicians in massachusetts. J Am Dent Assoc 2009; 140(4): 461-467.
12. Clovis JB, Horowitz AM, Poel DH. Oral and pharyngeal cancer: practices and opinions of dentists in British Columbia and Nova Scotia. J Can Dent Assoc 2002; 68(7): 421-25.
13. Lopez-Jornet P, Camacho-Alonso F, Moliva-Minano F. Knowledge and attitudes about oral cancer among dentists in Spain. J Eval Clin Pract 2010; 16(1): 129-33.
14. Patton LL, Elter JR, Southerland JH, Strauss RP. Knowledge of oral cancer risk factors and diagnostic concepts among North Carolina Dentists. Implications for diagnosis and referral. J Am Dent Assoc 2005; 136(5): 602-10.
15. Gajendra S, Cruz GD, Kumar JV. Oral cancer prevention and early detection knowledge, practices, opinions of oral health care providers in New York State. J Cancer Educ 2006; 21(3): 157-62.
16. Lehew CW, Kaste LM. Oral cancer prevention and early detection knowledge and practices of Illinosis dentists – a brief communication. J Public Health Dent 2007; 67(2): 89-93.
17. Hertrampf K, Wiltbang J, Koller M, Klosa K, Wenz HJ. Dentist perspectives on oral cancer: a survey in Northern Germany and a comparison with international data. Eur J Cancer Prev 2010; 19: 144-52.
18. Alonge OK, Narendran S. Oral cancer knowledge and practices of dentists along the Texas- Mexico Border. J Cancer Educ 2004; 19: 16-11.
19. Sanskaranaryan R, Ramadas K, Thomas G, Muwonge R, Thora S, Mathew B, Rajan B. Trivandrum oral cancer screening study group: Effect of screening on oral cancer mortality in Kerala, India: a cluster – randomised controlled trial. Lancet 2005; 365: 1927-33.
20. Scully C, Porter S. ABC of oral health swellings and red, white and pigmented lesions. BMJ 2000; 321(7255): 225-28.
21. Reichart PA, Philipsen HP. Oral erythroglakia-a review-oral oncol 2005; 41: 551-61.
22. McCann M, Macpherson L, Gibson J. The role of the general dental practitioner in detection and prevention of oral cancer: a review of literature. Dent Update 2000; 27: 40-8.
23. Miller PM, Ravenel MC, Shealy AE, Thomas S. Alcohol screening in dental patients: the prevalence of hazardous drinking and patients attitudes about screening and advice. J Am Dent Assoc 2006; 137: 1692-98.
|